
Additional pediatric resources: GeneralPediatrics.com | PediatricEducation.org | SearchingPediatrics.com
Donna M. Santer, M.D., Michael P. D'Alessandro, M.D.
Peer Review Status: Externally Peer Reviewed by Lauren D
Holinger, MD, Robert J. Winter, MD and the AMA
Of these four, the larynx, especially its subglottic region, is the most common site because this is the narrowest point of the pediatric airway. The causes of subglottic stenosis may be divided into congenital or acquired lesions, and these will be considered separately because of the differences in pathophysiology, evaluation, and treatment of each.
Congenital Subglottic Stenosis
Congenital subglottic stenosis is defined as subglottic stenosis in
the absence of a history of intubation, other laryngeal trauma, or
extrinsic compression, such as a vascular malformation like a double
aortic arch. The child may present at birth, in the neonatal period,
or in the first few weeks or months of life. It is caused by failure
to recanalize the lumen of the larynx and trachea in embryonic life,
thus resulting in atresia, webs
![]() , or
stenosis. Not unexpectedly, there is an increased incidence of other
lesions in the airway if one area is already affected.
, or
stenosis. Not unexpectedly, there is an increased incidence of other
lesions in the airway if one area is already affected.
The children appear reasonably well with normal growth and development, but they come to the physician's attention because of stridor. The stridor may have an expiratory component as well as the normal inspiratory component , ie, biphasic (SOUND). The child may also present with dyspnea, a brassy or barky cough, hoarseness, and/or weak or unusual cry. A prolonged episode or unusual course of croup may also bring the child to attention.
The physical examination findings depend on the amount of
obstruction in the airway. The child may have only a minimal amount
of obstruction, and normally may be without symptoms. But obstruction
of the airway may rapidly increase when the edema caused by an URI is
superimposed on the already compromised airway. For example, 1 mm of
edema in the subglottic region will decrease the cross-sectional area
of the airway by over 50%
![]() .
Obviously, if the original obstruction is severe, the child will
present early and with more severe symptoms, including presentation
of stridor in the delivery room
(SUMMARY)
(SUMMARY).
.
Obviously, if the original obstruction is severe, the child will
present early and with more severe symptoms, including presentation
of stridor in the delivery room
(SUMMARY)
(SUMMARY).
Evaluation of the child with possible congenital subglottic
stenosis may include the use of endolateral neck x-rays to look for
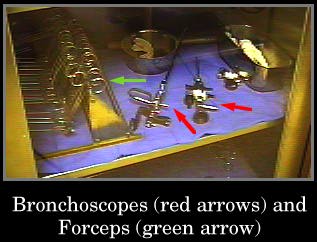
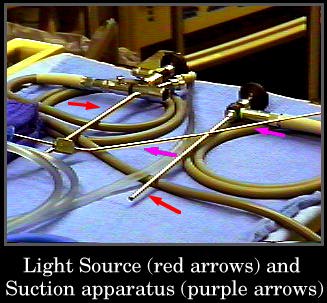
narrowing in the subglottic region. Bronchoscopy, or the more correct
term laryngoscopy if only the laryngeal structures are visualized, is
needed for complete evaluation of the airway, to rule out other
anomalies, and for definitive diagnosis
(SUMMARY)
![]()
![]()
![]()
![]() .
Bronchoscopy shows marked soft tissue swelling 2-3 mm below the vocal
cords. Occasionally, the lumen is eccentric with greater involvement
of one area of the wall.
.
Bronchoscopy shows marked soft tissue swelling 2-3 mm below the vocal
cords. Occasionally, the lumen is eccentric with greater involvement
of one area of the wall.
Treatment of the disorder is based on etiology and amount of
obstruction. Most children outgrow their subglottic stenosis and
require only expectant watching. Occasionally, repeat bronchoscopy
for evaluation of progress is needed. Other children may require
periodic dilatation with tracheal dilators
![]() . Because
the inelastic cricoid cartilage allows only the inward swelling of
tissues, tracheotomy may be needed. This should be done with the
smallest size tracheostomy tube to allow adequate ventilation and
preservation of laryngeal function for speech. Operative
laryngo-tracheoplasties may also be needed in some children.
Aggressive supportive treatment including antibiotics,
corticosteroids, and occasionally mechanical ventilation, during
intercurrent illnesses, is also needed by these children. Generally,
they outgrow their stenosis by age 3 - 4 years
(SUMMARY). In
between these events, children with tracheostomies lead very normal
lives
. Because
the inelastic cricoid cartilage allows only the inward swelling of
tissues, tracheotomy may be needed. This should be done with the
smallest size tracheostomy tube to allow adequate ventilation and
preservation of laryngeal function for speech. Operative
laryngo-tracheoplasties may also be needed in some children.
Aggressive supportive treatment including antibiotics,
corticosteroids, and occasionally mechanical ventilation, during
intercurrent illnesses, is also needed by these children. Generally,
they outgrow their stenosis by age 3 - 4 years
(SUMMARY). In
between these events, children with tracheostomies lead very normal
lives ![]()
![]() . Even
tracheostomy tube changes cause little disruption of their daily
activities
. Even
tracheostomy tube changes cause little disruption of their daily
activities ![]() .
.
Differential diagnosis includes vascular malformations,
laryngomalacia, asthma, croup, or bronchiolitis. The complications of
the disorder are respiratory failure, with mechanical ventilation and
its concomitant complications
![]() , and
problems secondary to the tracheostomy itself, such as increased risk
of infections. It is interesting to note that these children do have
an increased risk of respiratory infections out of proportion to
normal children even accounting for problems such as having a
tracheostomy.
, and
problems secondary to the tracheostomy itself, such as increased risk
of infections. It is interesting to note that these children do have
an increased risk of respiratory infections out of proportion to
normal children even accounting for problems such as having a
tracheostomy.
Acquired Subglottic Stenosis
Acquired subglottic stenosis is caused by trauma to the subglottic
structures secondary to endotracheal intubation but also due to a
foreign body, infection, or chemical irritation. The respiratory
epithelium is very susceptible to irritation, and, if it persists,
the original edema and hyperemia progress to ulceration and local
infection with growth of granulation tissue
![]() . If
irritation still persists, destruction of the underlying cricoid
cartilage and other cartilaginous supports occur. When the source is
finally removed and healing can take place, the scar tissue contracts
circumferentially producing a stricture or even complete stenosis.
The age of initial diagnosis varies considerably from 2 weeks to 10
years or more, with the majority being less than 1 year old.
. If
irritation still persists, destruction of the underlying cricoid
cartilage and other cartilaginous supports occur. When the source is
finally removed and healing can take place, the scar tissue contracts
circumferentially producing a stricture or even complete stenosis.
The age of initial diagnosis varies considerably from 2 weeks to 10
years or more, with the majority being less than 1 year old.
The clinical presentation and physical examination of children with acquired subglottic stenosis is the same as those of children with congenital subglottic stenosis. The history generally reveals endotracheal intubation for a period of time or other insult such as a foreign body or chemical aspiration. If the cause is endotracheal intubation, the child may present with inspiratory stridor just a few hours after extubation.
Evaluation of these children also begins generally with
endolateral neck x-rays that reveal various amounts of subglottic
narrowing. The narrowing can be severe with a steeple sign similar to
that of croup, but it is most often can be subtle. Bronchoscopy,
however, shows more severe stenosis than is found in congenital
subglottic stenosis. Circumferential stenosis with an associated web
or band is often noted. Vocal cord paralysis may also be seen
![]() .
.
Treatment of these children needs to be more aggressive, because
the problem is usually more severe than with congenital stenosis. If
the child presents within a few hours of extubation, racemic
epinephrine nebulization may be all that is needed. Frequent arterial
blood gas analysis for monitoring of hypercarbia and possible
respiratory failure may be futile as many children have normal blood
gas analysis until they are in frank failure. If the child shows
progressive symptoms, reintubation may be necessary and a course of
corticosteroids should be used before the next attempt to extubate.
For those children who fail this second attempt at extubation, a
surgical procedure is indicated. A cricoid split tracheoplasty or
laser surgery ![]() may be
used to avoid tracheotomy, depending on the individual clinical
indications. Many more children require tracheotomy for acquired
subglottic stenosis than those with the congenital type. They also
require repeat dilatation
may be
used to avoid tracheotomy, depending on the individual clinical
indications. Many more children require tracheotomy for acquired
subglottic stenosis than those with the congenital type. They also
require repeat dilatation
![]() and/or
endoscopic removal of granulation tissue more often. Children with
tracheostomies do well and can be decannulated in 1-2 years. These
children tend to have a higher morbidity and mortality due to their
underlying disease such as hyaline membrane disease and have longer
hospitalizations
(SUMMARY).
and/or
endoscopic removal of granulation tissue more often. Children with
tracheostomies do well and can be decannulated in 1-2 years. These
children tend to have a higher morbidity and mortality due to their
underlying disease such as hyaline membrane disease and have longer
hospitalizations
(SUMMARY).
The differential diagnosis and complications for acquired subglottic stenosis are the same as those for congenital subglottic stenosis.
Conclusion
Subglottic stenosis is a common cause of stridor and airway
compromise in the pediatric population
(TABLE). The key
points are:
Questions About Subglottic Stenosis
1. Where is the narrowest part of the pediatric airway? The adult
airway? (ANSWER)
2. What is the basis for the cause of congenital subglottic stenosis in embryonic life? (ANSWER)
3. Congenital subglottic stenosis generally presents at what age and with what symptom? (ANSWER)
4. List three major options for treatment of congenital subglottic stenosis. (ANSWER)
5. List two infectious disease processes that may masquerade as congenital subglottic stenosis. (ANSWER)
6. How is the acquired form of subglottic stenosis caused? (ANSWER)
7. On bronchoscopy, acquired subglottic stenosis has more stenosis than the congenital form. What other anomalies may be seen? (ANSWER)
8. What other interventions may be tried with a child with subglottic stenosis who has failed extubation before a surgical procedure is done? (ANSWER)
Next Page | Previous Page | Title Page
Additional pediatric resources: GeneralPediatrics.com | PediatricEducation.org | SearchingPediatrics.com
Please send us comments by filling out our Comment Form.
All contents copyright © 1992-2024 Donna M. D'Alessandro, M.D. and Michael P. D'Alessandro, M.D. and the authors. All rights reserved.
"Virtual Pediatric Hospital", the Virtual Pediatric Hospital logo, and "A digital library of pediatric information" are all Trademarks of Donna M. D'Alessandro, M.D. and Michael P. D'Alessandro, M.D.
Virtual Pediatric Hospital is funded in whole by Donna M. D'Alessandro, M.D. and Michael P. D'Alessandro, M.D. Advertising is not accepted.
Your personal information remains confidential and is not sold, leased, or given to any third party be they reliable or not.
The information contained in Virtual Pediatric Hospital is not a substitute for the medical care and advice of your physician. There may be variations in treatment that your physician may recommend based on individual facts and circumstances.
URL: http://www.virtualpediatrichospital.org/
{kind=link}
{kind=link}
{kind=link}